Baker’s Cyst
Updated:
What is a Baker’s cyst?
A Baker’s cysts is a condition characterized by local swelling situated behind the knee and typically occurs as a result of, and in association with, knee joint injuries (such as a meniscal tear or knee osteoarthritis).
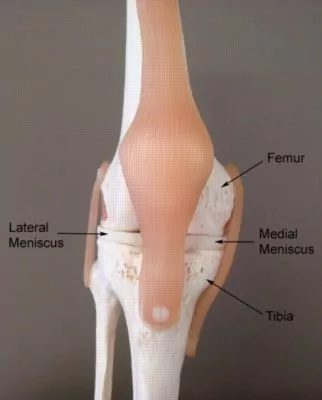
The knee joint comprises of the union of two bones: the long bone of the thigh (femur) and the shin bone (tibia) (figure 1). Between the bone ends are 2 round discs made of cartilage, called the medial (inner) and lateral (outer) meniscus (figure 1). Each meniscus acts as a shock absorber cushioning the impact of the femur on the tibia during weight-bearing activity. Wrapping around the entire knee joint is strong connective tissue known as the knee joint capsule which effectively forms a container within the knee joint. Behind the knee lie several small fluid filled sacs known as bursa. Bursa are designed to reduce friction between adjacent bony or soft tissue layers and often communicate with the knee joint.
Structures within the knee joint such as the medial and lateral meniscus may be damaged suddenly due to a specific incident or gradually over time due to repetitive or prolonged activities placing strain on tissue. This may be due to excessive weight bearing or twisting forces, a fall or an awkward landing from a height and may over time lead to knee osteoarthritis. When injury occurs to structures within the knee joint such as the menisci, swelling typically accumulates within the knee joint capsule and sometimes into the bursa (usually at the back of the knee) that communicate with the knee joint. This condition is known as a Baker’s cyst.
Causes of a Baker’s cyst
A Baker’s cyst most commonly occurs secondary to degenerative changes to the knee (knee osteoarthritis) or meniscal injuries (either acutely or due to gradual overuse). Meniscal injuries often occur traumatically in sports that require sudden changes of direction and twisting movements (sometimes in combination with excessive straightening or bending of the knee). These sports may include football, soccer, basketball, netball and snow skiing. Meniscal tears frequently take place when the foot is fixed on the ground and a twisting force is applied to the knee (e.g. when another player’s body falls across the leg, or when a player is tackled) or following a forceful jump or landing.
Meniscal injuries may also occur over time through gradual wear and tear associated with overuse (e.g. excessive distance running). This may be associated with, or lead to, degenerative changes within the knee joint over time (osteoarthritis), particularly in older patients.
Signs and symptoms of a Baker’s cyst
Patients with a Baker’s cyst typically experience a firm, lumpy swelling located at the back of the knee. In patients with a minor Baker’s cyst little or no symptoms may be present. As the condition worsens patients may experience pain or an ache located at the back of the knee and often a feeling of tightness, particularly when attempting to bend or straighten the knee fully. Sometimes this tightness may extend into the calf. Tenderness may also be experienced when firmly touching the Baker’s cyst at the back of the knee.
Patients with a Baker’s cyst may also experience other symptoms associated with the underlying cause of the Baker’s cyst. These symptoms may include clicking, grinding, locking, sharper pains, an audible sound at the time of injury, pain during certain activities (such as weight bearing activity, kneeling, twisting or squatting), knee weakness or collapsing, night or morning pain or ache, and, a limp or inability to weight bear on the affected limb.
Diagnosis of a Baker’s cyst
A thorough subjective and objective examination from a physiotherapist is usually sufficient to diagnose a Baker’s cyst and the underlying cause of the condition. An ultrasound investigation is usually the most appropriate investigation to identify the presence of a Baker’s Cyst. Other investigations, such as X-ray, MRI and CT scan are sometimes used to assist or confirm diagnosis and to determine the cause of the Baker’s cyst. In rare cases, where appropriate investigations have proven inconclusive, an investigative arthroscope may be performed to assist with diagnosis.
Treatment for a Baker’s cyst
Treatment for a Baker’s cyst of the knee primarily involves treatment of the underlying cause of the condition. Some Baker’s cysts may require no treatment and cause little or no symptoms.
Generally, patients with this condition should diligently follow the R.I.C.E. regime in the first 48 – 72 hours of injury. The R.I.C.E. regime can help to hasten healing and reduce pain and swelling and should comprise of rest from aggravating activities (crutches or a brace may be required), regular icing, the use of a compression bandage and keeping the leg elevated above the level of the heart. Anti-inflammatory medication may also help to hasten healing and recovery by reducing the pain and swelling associated with inflammation.
Patients with a Baker’s cyst should perform pain free flexibility and strengthening exercises as part of their rehabilitation to ensure an optimal outcome. One of the key components of rehabilitation is pain free strengthening of the quadriceps (vastus medialis obliquus muscle – VMO), hamstrings, gluteals and calf to improve the control of the knee joint with weight bearing activities. The treating physiotherapist can advise which exercises are most appropriate for the patient and when they should be commenced.
In patients who are not responsive to appropriate physiotherapy treatment, drainage of the bakers cyst (aspiration) followed by injection of a corticosteroid to reduce inflammation may help to settle the condition and hasten recovery. In rare cases surgery to the Baker’s cyst may be indicated.
Detailed information on the treatment of some common causes of a Baker’s cyst can be found in the links below:
Surgery for a Baker’s cyst
Despite appropriate physiotherapy management, a small percentage of Baker’s cysts may continue to cause significant discomfort and fail to improve with appropriate treatment. In these cases, surgery may be required to remove the Baker’s cyst and ensure an optimal outcome. The treating physiotherapist and doctor will refer to a specialist if surgery may be indicated. Physiotherapy and rehabilitation is then required following surgery to ensure an optimal outcome and enable a safe return to sport or activity.
Prognosis of a Baker’s cyst
Most patients with a Baker’s cyst heal well with appropriate physiotherapy and can often return to sport or activity in a number of weeks. Many cases may require no specific treatment.
In rare cases of this condition where patients experience significant discomfort and ongoing symptoms despite appropriate physiotherapy treatment, surgery may be indicated with a lengthy rehabilitation period to follow, lasting weeks to months.
Physiotherapy for a Baker’s cyst
Physiotherapy treatment is vital to hasten the healing process and ensure an optimal outcome in all patients with a symptomatic Baker’s cyst and is recommended in all patients with this condition regardless of whether they have surgery.
Physiotherapy treatment may comprise:
- soft tissue massage
- electrotherapy
- taping or bracing to support the knee
- mobilization
- dry needling
- hydrotherapy
- the use of crutches
- ice or heat treatment
- progressive exercises to improve flexibility, balance and strength (especially the VMO muscle)
- activity modification advice
- education
- biomechanical correction
- the prescription of orthotics
- anti-inflammatory advice
- weight loss advice where appropriate
- the use of Real-Time Ultrasound to assess and retrain the VMO muscle
- a gradual return to activity program
For those patients who are undergoing surgery to remove the Baker’s cyst, physiotherapy and rehabilitation should commence prior to surgery. This may include treatment to reduce pain and swelling, electrotherapy, strengthening and range of movement exercises, the use of a compression bandage, and the use of crutches etc.
Following surgery, physiotherapy and rehabilitation is essential to assist the healing process and ensure an optimal outcome.
In the final stages of rehabilitation for all patients with this condition, the physiotherapist can devise an appropriate return to sport or activity plan. Returning to activity too soon or without adequate rehabilitation will often lead to knee swelling and injury reoccurrence.
Other intervention for a Baker’s cyst
Despite appropriate physiotherapy management, some patients with a Baker’s cyst fail to improve either conservatively or following surgery. When this occurs the treating physiotherapist or doctor can advise on the best course of management. This may include further investigations, pharmaceutical intervention, corticosteroid injection, or further surgery.
Exercises for a Baker’s cyst
The following exercises are commonly prescribed to patients with a Baker’s cyst. You should discuss the suitability of these exercises with your physiotherapist prior to beginning them. Generally, they should be performed 3 times daily and only provided they do not cause or increase symptoms.
Knee Bend to Straighten
Bend and straighten your knee as far as possible without increasing your pain (figure 2). This helps to restore your normal knee movement. Repeat 20 times.

Static Quadriceps Contraction
Tighten the muscle at the front of your thigh (quadriceps) by pushing your knee down into a towel (figure 3). Put your fingers on your inner quadriceps to feel the muscle tighten during contraction. Hold for 5 seconds and repeat 10 times as hard as possible without increasing your symptoms.

Physiotherapy products for a Baker’s cyst
Some of the most commonly recommended products by physiotherapists to hasten healing and speed recovery in patients with a Baker’s cyst include:





To purchase physiotherapy products for a Baker’s cyst click on one of the above links or visit the PhysioAdvisor Shop.
Find a Physio for a Baker’s cyst
Find a Physiotherapist in your local area who can treat a Baker’s cyst and the underlying cause of the condition.
More Information
- View more Knee Strengthening Exercises
- View Knee Stretches
- View How To Use Crutches
- Read about Medial Meniscal Tears
- Read about Lateral Meniscal Tears
- Read about Knee Osteoarthritis
- Read about the R.I.C.E. regime

Link to this Page
If you would like to link to this article on your website, simply copy the code below and add it to your page:
<a href="https://physioadvisor.com.au/injuries/knee/bakers-cyst”>Baker’s Cyst – PhysioAdvisor.com</a><br/>PhysioAdvisor offers detailed physiotherapy information on a medial meniscus tear including signs and symptoms, causes, diagnosis, treatment, exercises and physiotherapy products.
Return to the top of Baker’s Cyst.