Shin Splints
Updated:
(Also known as Medial Tibial Tenoperiostitis, MTSS, Medial Tibial Stress Syndrome, Tenoperiostitis of the Shin, Inflammatory Shin Pain, Traction Periostitis, Posterior Shin Splint Syndrome)
What are shin splints?
Shin Splints (Medial Tibial Tenoperiostitis) is a condition characterized by damage and inflammation of the connective tissue joining muscles to the inner shin bone (tibia).
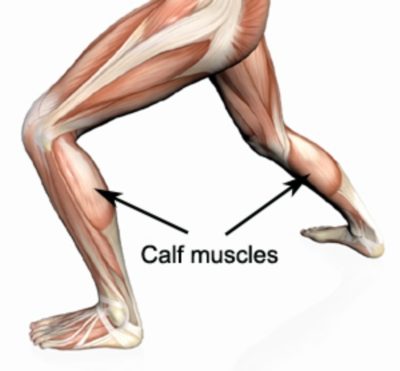
There are several muscles which lie at the back of your lower leg and are collectively known as the calf muscles (figure 1). Several of these muscles lie deep within the calf (tibialis posterior, flexor digitorum longus, flexor hallicus longus and soleus) and attach to the inner border of the shin bone (tibia). The connective tissue responsible for attaching these muscles to the tibia is known as the tenoperiosteum. Every time the calf contracts, it pulls on the tenoperiosteum. When this tension is too forceful or repetitive, damage to the tenoperiosteum occurs. This results in inflammation and pain and is known as medial tibial tenoperiostitis – commonly referred to as shin splints.
Medial tibial tenoperiostitis can sometimes occur in combination with other pathologies that cause shin pain such as compartment syndrome and tibial stress fractures.
Causes of shin splints
Shin splints most commonly occur due to repetitive or prolonged activities placing strain on the tenoperiosteum. This typically occurs due to excessive walking, running or jumping activities (such as an increase in training or running) and is often seen in runners and footballers. It frequently occurs in association with calf muscle tightness or biomechanical abnormalities, such as excessive pronation (flat feet – figure 2) or supination (high arch) or in those with inappropriate footwear. Athletes more commonly develop this condition early in the season following a period of reduced activity (deconditioning) and when training surfaces are generally harder.

Signs and symptoms of shin splints
Patients with shin splints typically experience pain along the inner border of the shin. In less severe cases, patients may only experience an ache or stiffness along the inner aspect of the shin that increases with rest (typically at night or first thing in the morning) following activities which place stress on the tenoperiosteum. These activities typically include excessive walking, running (especially up hills, on uneven surfaces or in poor footwear such as thongs), jumping and general weight bearing activity. The pain associated with this condition may also warm up with activity in the initial stages of injury. As the condition progresses, patients may experience symptoms that increase during sport or activity, affecting performance. In severe cases, patients may walk with a limp although this may also reduce to some extent as the patient warms up.
Patients with this condition typically experience pain on firmly touching the inner border of the shin bone particularly along the lower third of the bone. Areas of muscle tightness, thickening or lumps may also be felt in the area of pain. In severe cases, swelling, redness and warmth may also be present.
Diagnosis of shin splints
A thorough subjective and objective examination from a physiotherapist is usually sufficient to diagnose shin splints. Occasionally, further investigations such as an X-ray, ultrasound, bone scan, CT scan, MRI or compartment pressure testing may be used to assist diagnosis and rule out other conditions, such as compartment syndrome and tibial stress fractures.
Treatment for shin splints

Members Only ContentBecome a PhysioAdvisor Member to gain full access to this exclusive content. For more details see Become a Member. Already a member? Login Now
Prognosis of shin splints
Most patients with this condition heal well with appropriate treatment. Recovery time may range from a few weeks to many months depending on the severity of injury, quality of treatment and length of time the injury has been present for. Patients with shin splints that have been present for months may require a considerable period of treatment associated with reduced activity before full recovery occurs.
Contributing factors to the development of shin splints
There are several factors which can predispose patients to developing this condition. These need to be assessed and corrected with direction from a physiotherapist. Some of these factors include:
- excessive training or activity
- poor foot posture (especially flat feet – figure 2)
- inappropriate footwear
- inadequate warm up
- training on hard or inappropriate surfaces
- muscle weakness (especially the calf muscles)
- tightness in specific joints (such as the ankle)
- tightness in specific muscles (especially the calfs)
- poor lower limb biomechanics
- poor training technique or methods
- leg length differences
- poor balance
- being overweight
- deconditioning
- poor core stability
Physiotherapy for shin splints
Physiotherapy treatment for patients with this condition is vital to hasten the healing process, ensure an optimal outcome and reduce the likelihood of recurrence. Treatment may comprise:
- deep tissue massage (particularly to the calf muscles)
- joint mobilization
- dry needling
- electrotherapy
- PNF stretches
- arch support taping
- the use of orthotics or shock absorbing insoles
- the use of crutches
- biomechanical correction
- ice or heat treatment
- progressive exercises to improve flexibility (especially of the calf muscles), balance, strength and core stability
- activity modification advice
- anti-inflammatory advice
- footwear advice
- weight loss advice where appropriate






Other intervention for shin splints
Despite appropriate physiotherapy management, some patients with shin splints do not improve. When this occurs the treating physiotherapist or doctor can advise on the best course of management. This may include pharmaceutical intervention, further investigations such as X-rays, bone scan, CT scan, MRI, or compartment pressure testing, or a referral to an orthopaedic specialist who will advise on any procedures that may be appropriate to improve the condition. A review with a podiatrist may also be indicated for the prescription of orthotics to correct any foot posture abnormalities.
Exercises for shin splints
The following exercises are commonly prescribed to patients with this condition. You should discuss the suitability of these exercises with your physiotherapist prior to beginning them. Generally, they should be performed 2 – 3 times daily and only provided they do not cause or increase symptoms.
Your physiotherapist can advise when it is appropriate to begin the initial exercises and eventually progress to the intermediate and advanced exercises. As a general rule, addition of exercises or progression to more advanced exercises should take place provided there is no increase in symptoms.
Initial Exercises
Calf Stretch with Towel
Begin this stretch in long sitting with your leg to be stretched in front of you. Your knee and back should be straight and a towel or rigid band placed around your foot as demonstrated (figure 3). Using your foot, ankle and the towel, bring your toes towards your head until you feel a stretch in the back of your calf, Achilles tendon or leg. Hold for 5 seconds and repeat 10 times at a mild to moderate stretch provided the exercise is pain free.

Resistance Band Calf Strengthening
Begin this exercise with a resistance band around your foot as demonstrated and your foot and ankle held up towards your head (figure 4). Slowly move your foot and ankle down against the resistance band as far as possible and comfortable without pain, tightening your calf muscle. Very slowly return back to the starting position. Repeat 10 – 20 times provided the exercise is pain free.

Intermediate Exercises
Members Only ContentBecome a PhysioAdvisor Member to gain full access to this exclusive content. For more details see Become a Member. Already a member? Login Now
Advanced Exercises
Members Only ContentBecome a PhysioAdvisor Member to gain full access to this exclusive content. For more details see Become a Member. Already a member? Login Now
Other Exercises
Members Only ContentBecome a PhysioAdvisor Member to gain full access to this exclusive content. For more details see Become a Member. Already a member? Login Now
Rehabilitation Protocol for Shin Splints
The following is a general rehabilitation protocol for patients with shin splints. This needs to be tailored to each individual and should be discussed with your treating physiotherapist prior to commencing. Progression through this program can vary from weeks to many months depending on the injury severity, quality of treatment and duration the injury has been present for:
- See your physiotherapist as soon as possible to confirm diagnosis, establish the likely prognosis, identify the contributing factors to injury and begin appropriate treatment.
- Follow the R.I.C.E. Regime for the first 48 – 72 hours. This should primarily comprise:
- Rest from any activity that increases pain (if walking is painful or causing a limp, crutches are usually required). Appropriate footwear (including potential orthotics) is also important to reduce stress on the shin.
- Ice the sore area for 20 minutes and repeat every 2 hours (using an ice pack). Or alternatively, perform an ice massage using a polystyrene cup for 5 – 10 minutes every 2 hours).
- Compress the affected area using a compression bandage.
- Elevate the affected leg above the level of your heart whenever possible
- Anti-inflammatory medication may be beneficial (discuss this with your doctor and / or pharmacist)
- If using crutches, walk normally, but take enough weight off the injured leg so walking is pain free and limp free. Sometimes smaller steps may be required for a period of time. Gradually increase weight through the injured side as tolerated provided there is no increase in pain or limp.
- Aim for pain free rehabilitation (i.e. gradually increase strength, flexibility and activity, provided there is no increase in symptoms during activity or upon rest following activity (particularly the next night or morning). This should take place over a number of weeks).
- Begin “Initial Exercises” 72 hours following injury provided there is no increase in symptoms.
- Heat treatment can usually commence 72 hours following injury provided there is no inflammation (i.e. night-time pain, morning ache / stiffness or pain at rest). Apply a heat pack to the injured area at a comfortable warmth for 20 – 30 minutes before exercises. If inflammation is still present (i.e.night-time pain, morning ache / stiffness or pain at rest) continue to use ice instead of heat.
- Increase walking distance, and eventually speed, gradually, and, provided there is no increase in pain or limp (this should take place over a number of weeks).
- Progress to the “Intermediate Exercises” once the “Initial Exercises” can be performed pain free and to the same extent on the injured side as the non-injured side. Ensure all new exercises do not increase symptoms. The ‘Intermediate Exercises’ should replace the ‘Initial Exercises’. Generally you should begin with one ‘Intermediate Exercise’ and slowly add the remaining ‘Intermediate Exercises’ over a number of days provided there is no increase in symptoms.
- ‘Other Exercises’ may be added provided they do not cause or increase pain.
- Progress to the “Advanced Exercises” once the “Intermediate Exercises” can be performed pain free and to the same extent on the injured side as the non-injured side. Ensure all new exercises do not increase symptoms. The ‘Advanced Exercises’ should replace the ‘Intermediate Exercises’ and can be added to the ‘Other Exercises’. Generally you should begin with one ‘Advanced Exercise’ and slowly add the remaining ”Advanced Exercises’ over a number of days provided there is no increase in symptoms.
- Assessment with a podiatrist may be required for possible orthotics or footwear advice, particularly in patients with flat feet or high arches.
- A gradual Return to Running Program should be implemented for individuals who aim to return to running or running sports following injury provided there is no increase in symptoms.
- A gradual return to sport and activity can occur provided there is no increase in symptoms.
- Ensure your physiotherapist has identified the contributing factors to your injury and appropriate intervention has taken place to address these issues to minimize the likelihood of injury recurrence.
Other exercises
- View more Ankle Stretches.
- View more Ankle Strengthening Exercises.
- View more Calf Strengthening Exercises.
- View more Calf Stretches.
- View more Balance Exercises.
 Find a physiotherapist
Find a physiotherapist
Find a physiotherapist in your local area who can treat shin splints.
 Physiotherapy products for shin splints
Physiotherapy products for shin splints
Some commonly recommended products by physiotherapists for patients with this condition include:



To purchase physiotherapy products to assist with rehabilitation click on one of the above links or visit the PhysioAdvisor Shop.
 More information
More information
- View detailed information on How to use Crutches.
- View detailed information on when to use Ice or Heat.
- View detailed information on initial injury management and the R.I.C.E. Regime.
- View detailed information on a Return to Running Program.
- View detailed information on Do i need Orthotics.
- View detailed information on Choosing a Shoe.
- View detailed information on Foot Taping Techniques.
- View our Lower Leg Diagnosis Guide.
Become a PhysioAdvisor Member
-
 Individual Membership (12 Months)$59.95 for 1 year
Individual Membership (12 Months)$59.95 for 1 year -
Individual Membership (3 Months)$39.95 for 3 months
-
Individual Membership (Yearly)$49.95 / year
-
Individual Membership (Monthly)$15.95 / month

Link to this Page
If you would like to link to this article on your website, simply copy the code below and add it to your page:
<a href="https://physioadvisor.com.au/injuries/lower-leg/shin-splints”>Shin Splints – PhysioAdvisor.com</a><br/>We offer detailed physiotherapy information on Shin Splints and Shin Pain including causes, signs and symptoms, diagnosis, treatment, exercises and more.
Return to the top of Shin Splints.