Swimming Injuries
Updated:
Swimming is one of the most popular low-impact fitness activities. Although the most common complaint from swimmers is shoulder pain, a number of other areas of the body are sometimes injured from swimming, such as the neck, lower back and knees (depending on the type of stroke). Swimming injuries are typically ‘overuse’ and can affect either one or both sides of the body.

Most Common Swimming Injuries
Shoulder
Swimmers Shoulder (Rotator Cuff Tendonitis)
Degeneration and inflammation of one or more of the rotator cuff tendons (figure 1), often due to overuse or poor technique. Typically causes a pain or ache in the shoulder or upper arm which is often aggravated during swimming (particularly butterfly or front crawl strokes) or after swimming with rest (e.g. the next night / morning). In less severe cases, symptoms may also warm up during swimming only to reoccur later with rest. Pain commonly increases during lifting activities (especially with the arm outstretched or above the head) or when lying on the affected side. Pain may also increase on firmly touching the affected rotator cuff tendon (figure 1).
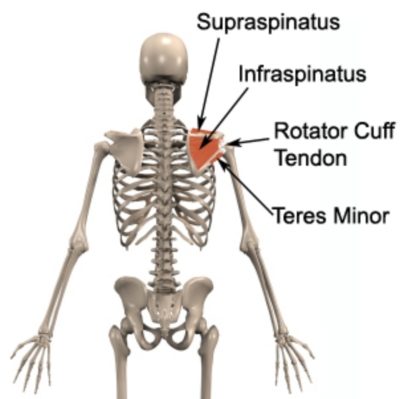
Figure 1 – Rotator Cuff Anatomy

Members Only ContentBecome a PhysioAdvisor Member to gain full access to this exclusive content. For more details see Become a Member. Already a member? Login Now
Neck
Members Only ContentBecome a PhysioAdvisor Member to gain full access to this exclusive content. For more details see Become a Member. Already a member? Login Now
Cervicogenic Headache
Headache originating from the neck typically as a result of damage to the joints located at the upper aspect of the neck, often as a result of repetitive or prolonged turning of the neck (e.g. breathing during swimming), slouching (especially during sitting, sleeping or use of a computer), bending forwards of the neck (e.g. tumble turns during swimming), shoulders forwards activities (such as breaststroke or butterfly) or lifting. Typically causes a constant, dull ache that may present in the back of the head, top of the forehead, behind the eye, in the temple region or less commonly, around the jaw or ear. Usually associated with neck pain, stiffness and difficulty turning the neck. Symptoms may also increase on firmly touching the affected level of the spine, usually on one side of the neck, just below the base of the skull. Occasionally other symptoms may be present such as pins and needles, numbness, dizziness, nausea or light headedness.
Lower Back
Lumbar Disc Bulge
Tearing of connective tissue surrounding a disc in the lower back with subsequent bulging of disc material (figure 7). Typically as a result of repetitive or prolonged bending forwards of the lower back (e.g. during tumble turns when swimming), during sitting, lifting or twisting or following trivial movements such as picking up a pencil or sneezing. May cause lower back pain centrally or on one or both sides of the spine, with or without symptoms radiating into the buttock, groin, thigh, lower leg, ankle or foot. Pain may increase on firmly touching the affected level of the spine and there is often associated muscle spasm and restricted spinal movement. Occasionally there may be no lower back pain, with only symptoms down the affected leg. Pins and needles or numbness is occasionally present in the affected leg or foot. Symptoms often increase with repetitive or prolonged sitting, bending, lifting, coughing or sneezing and are often worse first thing in the morning.
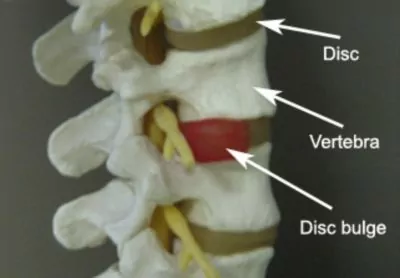
Figure 7 – Lumbar Disc Bulge Anatomy
Members Only ContentBecome a PhysioAdvisor Member to gain full access to this exclusive content. For more details see Become a Member. Already a member? Login Now
Knee
Breaststrokers Knee (MCL Sprain)
Overuse tearing or inflammation of the medial collateral ligament of the knee (MCL – Figure 9), typically following repetitive breaststroke kicking. Often due to inadequate range of movement at the hip joints and associated with pain on firmly touching the inner aspect of the knee and an increase in pain during the breaststroke kick.
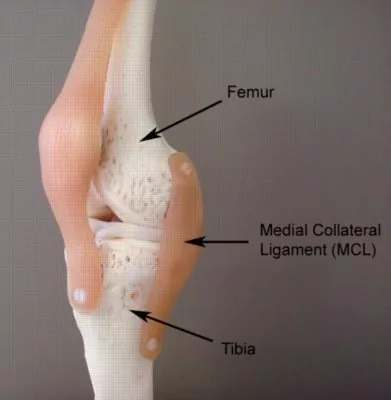
Figure 9 – MCL Anatomy
 Contributing Factors to Swimming Injuries
Contributing Factors to Swimming Injuries
A number of factors may contribute to the development of swimming injuries, including:
- Inadequate upper limb and shoulder flexibility (particularly shoulder flexion, abduction, external or internal rotation)
- Muscle tightness (particularly the latissimus dorsi, pectorals, rotator cuff, abdominals & hip flexors)
- Inadequate thoracic spine flexibility (particularly into extension and rotation)
Members Only ContentBecome a PhysioAdvisor Member to gain full access to this exclusive content. For more details see Become a Member. Already a member? Login Now
Injury Prevention Tips for Swimming Injuries
Members Only ContentBecome a PhysioAdvisor Member to gain full access to this exclusive content. For more details see Become a Member. Already a member? Login Now
Flexibility
Ensuring adequate flexibility is important to improve your stroke efficiency and minimise drag, thus reducing the risk of injury. Key joints which require adequate range of motion for swimming include:
- Shoulder
- Upper Back
- Hips
- Ankles
Flexibility Exercises for these body parts and the muscles surrounding them are an important aspect of injury prevention for swimmers. Massage Therapy to these areas can also play a key role in maintaining adequate range of movement (see upper body and lower body massage ball exercises).
Core Stability & Conditioning
Many swimming injuries can be attributed to poor strength or activation of the core stabilisers, such as the scapular stabilisers, rotator cuff, gluteals, transverses abdominis, obliques, multifidus and pelvic floor. As part of your training, ensure you spend enough time working on improving your core stability, rotator cuff strength and scapular stability (see Core Stability Exercises, Pilates Exercises and Rotator Cuff Exercises). A variety of activities that help develop total body conditioning, muscular strength, and muscular endurance is also essential. A land based (dry land) program should be implemented, including scapular and trunk stabilizing exercises, and, cross training exercises.
Training Appropriately
When increasing training workloads (such as at the start of the swimming season) make sure you increase your training distances, intensities or frequencies gradually to allow your body to absorb the increased workload. Follow the ‘10% Rule’ to minimise the risk of overuse injury. This means only increasing one variable (distance, time, intensity) by no more than 10% per week. Avoid long or high intensity swims on consecutive days. If you are swimming excessively long distances aim to have at least 48hrs between ‘heavy’ sessions to allow your body to recover. Use cross training sessions (e.g. cycling, running, rowing) to maintain your cardio workload without the risk of overuse injuries to the upper limb.
Members Only ContentBecome a PhysioAdvisor Member to gain full access to this exclusive content. For more details see Become a Member. Already a member? Login Now
 Physiotherapy Products for Swimming Injuries
Physiotherapy Products for Swimming Injuries
The following physiotherapy products are commonly prescribed to patients by physiotherapists to assist in the rehabilitation and prevention of swimming injuries:








To purchase physiotherapy products to assist in the rehabilitation and prevention of swimming injuries, click on one of the above links or visit the PhysioAdvisor Shop.

Link to this Page
If you would like to link to this article on your website, simply copy the code below and add it to your page:
<a href="https://physioadvisor.com.au/injury-diagnosis/sports-injuries/swimming-injuries”>Swimming Injuries – PhysioAdvisor.com</a><br/>PhysioAdvisor provides detailed physiotherapy information on swimming injuries including most common swimming injuries, contributing factors and injury prevention tips.
Return to the top of Swimming Injuries.