Supracondylar Fracture
Updated:
(Also known as a Fractured Humerus, Broken Humerus)
What is a supracondylar fracture?
A supracondylar fracture is a relatively uncommon condition involving a break in the upper arm bone (humerus – figure 1) just above the elbow joint.
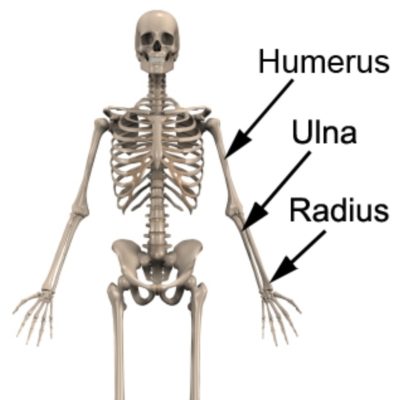
The elbow joint comprises the union of 3 long bones: the humerus (upper arm bone), the ulna and the radius (lower arm bones) (figure 1). The humerus has two bony prominences known as the epicondyles situated at the inner and outer aspect of the elbow. Just above the epicondyles is a region of the humerus bone known as the supracondylar region (figure 2).

Stress is placed on the humerus bone and supracondylar region during certain activities (such as a fall onto an outstretched hand). When these forces are traumatic and exceed the bone’s tolerance, a break in the supracondylar region of the humerus may result. When this occurs, the condition is commonly known as a supracondylar fracture.
A supracondylar fracture is more common in children than in adults. Often these humerus fractures occur in combination with other injuries such as a sprained or dislocated elbow or other fractures of the upper limb.
Supracondylar fractures vary in severity, location and nature. Their classification and type may include:
- greenstick fracture
- comminuted fracture
- displaced fracture
- un-displaced fracture etc.
Causes of a supracondylar fracture
A supracondylar fracture most commonly occurs due to a traumatic weight bearing force through an outstretched arm such as a fall from a height or bicycle. They may also occur due to a direct blow to the elbow or arm from a moving object or due to collision with a stationary object (such as road / traffic accidents or contact sports).
Signs and symptoms of a supracondylar fracture
At the time of injury, a supracondylar fracture typically causes a sudden onset of intense, often sharp, elbow or upper arm pain. This may cause the patient to cradle the affected arm to protect the injury. Sometimes, pain can settle relatively quickly leaving patients with an ache at the site of injury that is particularly prominent with rest (often at night or upon waking first thing in the morning).
Patients with this condition may also experience symptoms such as weakness, bruising, prominent swelling and pain on applying pressure to the fractured bone. The pain associated with this condition will typically increase during certain activities or movements of the elbow, wrist or shoulder or during weight-bearing activity (such as pushing) through the affected arm. Pins and needles or numbness may also be present in the elbow, forearm, hand or fingers. Clicking or grinding sensations are also sometimes experienced. In severe supracondylar fractures (with bony displacement), an obvious deformity at the fracture site may be detected.
Diagnosis of a supracondylar fracture
Examination by a physiotherapist or doctor is a vital component of diagnosis of supracondylar fractures. Further evaluation with an X-ray is needed to confirm the condition. Investigations such as a CT scan, MRI, or occasionally bone scan may be indicated, in some cases, to assist with diagnosis, determine the involvement of other structures and assess the fracture severity.
Treatment for a supracondylar fracture
Because supracondylar fractures are rotationally unstable and have a high rate of neurovascular complications, they should be considered an orthopaedic emergency. For those fractures that are unstable, displaced or cannot be reduced without jeopardizing the blood supply, treatment usually involves anatomical reduction (i.e. careful manipulation of the fracture under anesthetic to restore its anatomical alignment) followed by surgical external or internal fixation (e.g. using pins) to stabilise the fracture. This may be followed by the use of a splint, plaster cast, sling or brace for a number of weeks.
For isolated, non-displaced supracondylar fractures, treatment typically involves immobilization either via external or internal fixation, a splint or plaster cast for approximately 4 – 6 weeks.
The orthopaedic surgeon will determine the most suitable treatment for the fracture based on numerous factors such as the severity, type and location of the injury.
Follow up X-rays (at an appropriate interval) are important to evaluate the fracture and ensure healing is taking place in optimal alignment. Once confirmation of healing has been established and the plaster cast has been removed, rehabilitation can generally begin as instructed by the treating physiotherapist.
One of the key components of appropriate rehabilitation following a supracondylar fracture is to ensure that the patient rests from any activity that increases their pain. Activities that place prominent force through the humerus should also be avoided (in the early stages of healing) particularly lifting, weight bearing or pushing activities. Rest from aggravating activities allows healing to occur without further tissue damage. Once the fracture has regained sufficient strength and the patient can perform these activities without pain, a gradual return to these activities is appropriate provided there is no symptomatic increase. This return to activity should take place over a period of weeks to months and under physiotherapist guidance.
Adopting a ‘no pain, no gain’ attitude or ignoring symptoms is likely to cause further tissue damage and can slow or prevent healing of the fracture.
Pain-free, progressive, rehabilitation exercises are essential to restore flexibility and strength to the elbow and upper limb following a supracondylar fracture. This is important to ensure an optimal outcome and reverse any strength or flexibility losses (that quickly occur) with immobilisation. The treating physiotherapist will advise when exercises can commence and determine the most suitable exercises for the patient and stage of healing.
Prognosis of a supracondylar fracture
Most supracondylar fractures can expect a complete recovery with appropriate surgical or conservative management. Return to sport or activity can often occur after weeks to months and should be guided by the orthopaedic specialist and physiotherapist. In some cases involving severe injuries with associated damage to other structures (e.g. nerves, blood vessels, other bones or soft tissue) recovery periods can be markedly longer.
Physiotherapy for a supracondylar fracture
Appropriate physiotherapy management is important to speed recovery and ensure an ideal outcome in all patients with a supracondylar fracture. Treatment may entail:
- education
- activity modification advice
- exercises to restore flexibility, strength and function
- taping or bracing
- use of a sling
- the use of a compression bandage
- soft tissue massage
- joint mobilization
- electrotherapy (e.g. ultrasound)
- a graduated return to sport or activity plan




Other intervention for a supracondylar fracture
Some supracondylar fractures may not improve sufficiently despite appropriate rehabilitation and management. In these situations, other intervention may be indicated as guided by the treating physiotherapist or doctor. This may entail X-ray, MRI, CT or bone scan investigations, prolonged immobilisation in a plaster cast or referral to an orthopaedic specialist (or other relevant medical practitioners) who can determine the most appropriate course of management to optimise the condition. In rare cases, some supracondylar fractures that are initially managed conservatively may require surgical intervention to stabilize the fracture and a bone graft to enhance healing.
Exercises for a supracondylar fracture
The exercises outlined below are often prescribed to patients with a supracondylar fracture. This typically occurs once the orthopaedic specialist has indicated it is safe to begin mobilisation and after confirmation has been obtained that the fracture has healed sufficiently. The suitability of these exercises should be discussed with your physiotherapist prior to commencement. Generally, the exercises should be performed 3 times per day, provided they do not provoke or increase symptoms.
Elbow Bend to Straighten
Bend and straighten your elbow as far as possible pain free (figure 3). Aim for no more than a mild to moderate stretch. Repeat 10 times provided there is no increase in symptoms.
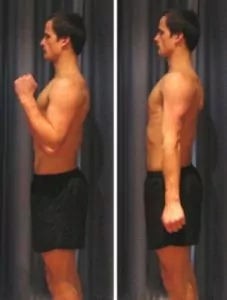
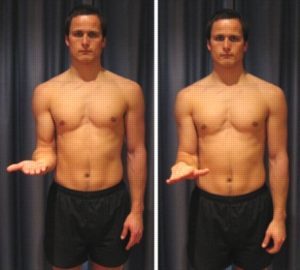
Forearm Rotations
Begin this exercise with your elbow at your side and bent to 90 degrees (figure 4). Slowly rotate your palm up and down as far as possible pain free. Aim for no more than a mild to moderate stretch. Repeat 10 times provided there is no increase in symptoms.
Tennis Ball Squeeze
Begin this exercise holding a tennis ball (figure 5). Squeeze the tennis ball as hard as possible and comfortable without pain. Hold for 5 seconds and repeat 10 times.

 Physiotherapy products for a supracondylar fracture
Physiotherapy products for a supracondylar fracture
Physiotherapy products that are commonly recommended to speed healing and hasten recovery following a supracondylar fracture include:
To purchase physiotherapist recommended products for a supracondylar fracture click on the relevant link above or visit the PhysioAdvisor Shop.
 Other Exercises
Other Exercises
- View more Elbow Stretches.
- View more Elbow Strengthening Exercises.
 Find a Physio for a supracondylar fracture
Find a Physio for a supracondylar fracture
Find a Physiotherapist who can treat a supracondylar fracture.
Become a PhysioAdvisor Member
-
 Individual Membership (12 Months)$59.95 for 1 year
Individual Membership (12 Months)$59.95 for 1 year -
Individual Membership (3 Months)$39.95 for 3 months
-
Individual Membership (Yearly)$49.95 / year
-
Individual Membership (Monthly)$15.95 / month

Link to this Page
If you would like to link to this article on your website, simply copy the code below and add it to your page:
<a href="https://physioadvisor.com.au/injuries/elbow-forearm/supracondylar-fracture”>Supracondylar Fracture – PhysioAdvisor.com</a><br/>PhysioAdvisor offers detailed physiotherapy information on a supracondylar fracture including: causes, symptoms, diagnosis, treatment, exercises, physiotherapy products and more...
Return to the top of Supracondylar Fracture.